Poop smarter (not harder): Does the Squatty Potty really work?
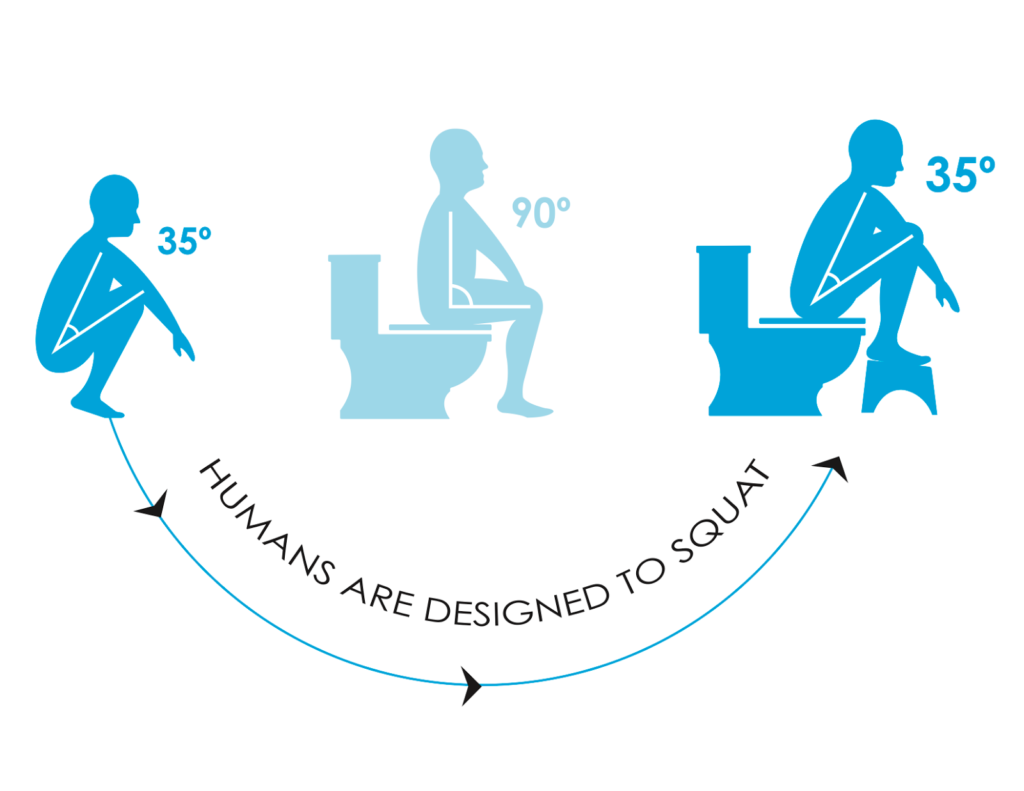
Does the #SquattyPotty really work? The truth is that it’s not the specific “Squatty Potty” step-stool that helps, it’s being in a squatting position that helps (i.e. any step-stool that helps your child be in a squatting position while having…

